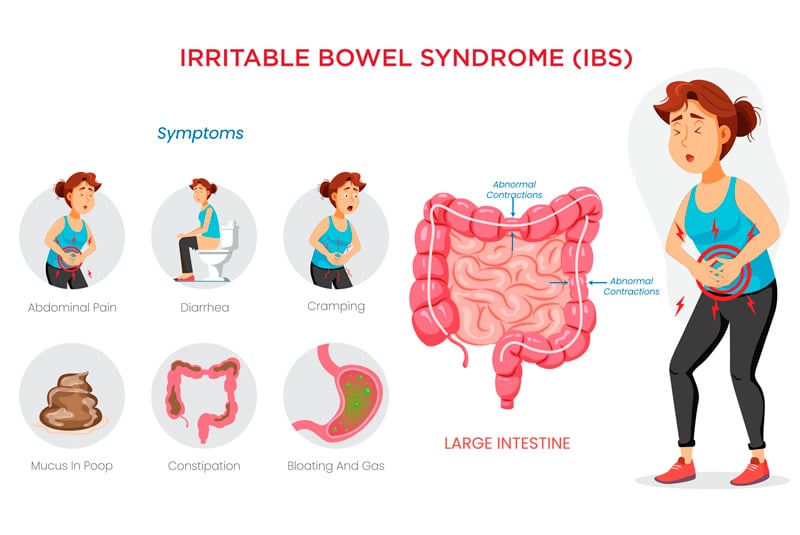
Irritable Bowel Syndrome (IBS) is a condition hallmarked by irregular or unpredictable bowel movements that occur with abdominal pain, bloating and gas. It’s not a structural issue of the bowel, rather a problem with the gut-brain axis (known as a ‘functional’ disorder); this means that the digestive tract looks normal on tests but does not behave as it should. It’s a condition that’s more common in people with high levels of stress, anxiety and trauma, and often significantly impacts the way that someone manages their day-to-day activities.
So what does IBS look like?
There are four types of IBS: IBS-D (diarrhoea predominant), IBS-C (constipation predominant), IBS-M (with mixed bowel habits) and IBS-U (unclassified). In IBS (not to be confused with IBD, which is inflammatory bowel disease), blood tests and faecal calprotectin tests come back normal, and colonoscopies show no structural damage.
Common symptoms include constipation or diarrhoea that feels like it doesn’t make sense, abdominal pain, wind and bloating. We don’t know exactly what causes such a constellation of symptoms in the absence of a single clear cause, but we do know what contributes;
The gut-brain axis is the complex communication network between your gastrointestinal tract, immune system and nervous system, and if it’s under (particularly prolonged) stress or exertion, it will start to let you know. There is a clear link between the health of your nervous system and gut motility, gas production and fermentation, bile acid production and systemic inflammation, which means the function of the gastrointestinal tract can change based on your mental health.
Most people can relate to doing a ‘nervous poo,’ but having IBS can feel like this 24/7. It’s important to remember that the thing that tells your body how to function IS your nervous system; they’re not separate, so good care of ‘central factors’ like sleep, stress, sedentary behaviour drives good gut function. The problem isn’t in your head, but it often does originate in the nervous system and ignoring these central drivers will often leave people frustrated at their physical symptoms as they don’t change, or just keep coming back no matter that you do.
We also know that an altered microbiome of the gut can drive dysregulation in the rest of your system, particularly through the gut-brain axis, and we know that many people with IBS do have a dysbiosis (an imbalance of the ‘good’ gut bacteria, or your ‘gut garden’). It can be triggered by a mental or physical illness, medication or dietary change or a hormonal change such as menstruation, pregnancy, menopause or puberty. It’s important to know that there is no one particular food that’s linked with developing IBS and triggers may look different for different people, but diet can be a critical part of its management.
There is thought to be a genetic component to the way your gut functions. If you are female and/or have a family history of IBS, you’re more likely to develop the condition.

So I have IBS — How do I manage it?
We see that with IBS of any type, pelvic floor function changes over time. It can be a ‘chicken or egg’ situation – is your pelvic floor holding on for dear life because your bowel is either overactive or full, or is your pelvic floor making it difficult to fully empty your bowels? Either way, pelvic physio is key to optimising your pelvic floor muscle function, creating strength to use when you need to hold on and facilitating a full relaxation of your muscles so you can pass stool completely.
Your physiotherapist will take a careful and complete history of your symptoms, examine you to find out whether your pelvic floor is helping or hindering you, and help you to train it to work for you, not against you.
Dietary management can be critical to manage symptoms of IBS, regardless of which subtype you have. Limiting or changing intake of trigger foods such as caffeine, alcohol, sweeteners, high FODMAP foods or spice may help, and looking at your fibre and fluid intake as well as the timing of your meals is key to making achievable changes that help your body function without unnecessarily restricting what you eat.
It’s also worth being looked after by a skilled and experienced multidisciplinary team that includes a gastroenterologist to rule out pathology or any medical underlying causes, dietitian to help manage your triggers and gut microbiome health, and importantly, a pelvic health physiotherapist to help guide your nervous system to a regulated state and manage any pelvic floor muscle dysfunction you’re experiencing, so your ‘mechanics’ function the way they should.
Your GP will also organise any other specialist referrals including to a gynaecologist or psychologist, depending on your other symptoms and contributing factors.
If you’re not sure where to start, come and see us at SPC. We work with a highly experienced team of pelvic physiotherapists and our network extends to a solid multidisciplinary team; we can help guide recommendations so you find the right people to help you. A collaborative approach helps with symptom management, allows you to regain control and stop letting your bowels run your day.
It’s important to have an individualised care plan to address your contributing factors, as we know they’re not the same in everyone (so ChatGPT probably shouldn’t take it from here!)
Contact us to book an appointment
Links
References: