This article seeks to explain the broader, non-lesion contributors to pain and suggest ways to address them.
Endometriosis is derived from the Latin term ‘endo’ (inside), ‘metra’ (uterus) and ‘osis’ (disease). It is a complex, inflammatory, estrogen dependant pain disorder affecting 11% of women, girls and those assigned female at birth (1, 2). It is characterised by tissue similar to the lining of the uterus (endometrium) growing in other parts of the body, including around the bladder, bowel and it has also been found in the skin, lungs and brain (1, 3).
Common symptoms of endometriosis are period pain (dysmenorrhea), heavy bleeding (menorrhagia), infertility, fatigue, painful urination (dysuria), difficult defecation (dyschezia) and sexual pain (dyspareunia). The pain symptoms may be constant, intermittent, or provoked and the severity may fluctuate monthly, hourly or daily. It takes an average of 6.5 years to receive a diagnosis of endometriosis (4), and by this point, a person’s pain experience is often not accurately represented by the stage of disease (5). Meaning, women with the most severe Stage 4 endometriosis can experience minimal symptoms, where others with mild Stage 1 can be immensely impacted by pain. It can be a confusing experience for patients to undergo laparoscopic surgery, where all diseased tissue has been successfully removed, and menstruation is suppressed with hormonal or medical treatments yet their pain persists.
Typically, patients are left asking clinicians questions such as:
- Why do I still have pain after my endometriosis surgery?
- How can I still have pelvic and period pain even though I’m using hormone therapy to suppress my cycle?
- All my test results have come back normal…so why do I still have pain?
This article seeks to explain the broader, non-lesion contributors to pain and suggest ways to address them.
Endometriosis-Associated Pain (EAP) Syndrome
EAP syndrome is defined by 2023 European Association of Urology (EAU) Guidelines for Chronic Pelvic Pain as ‘persistent or recurrent pelvic pain in patients with laparoscopically confirmed endometriosis, and the term is used when the symptoms persist despite adequate endometriosis treatment. It is often associated with negative cognitive, behavioural, sexual or emotional consequences, as well as with symptoms suggestive of lower urinary tract, sexual, bowel or gynaecological dysfunction.’ (6) While Endometriosis is thought to initially arise due to local inflammation, lesions and hormonal effects (1), the persistent nature of EAP is due to a more widespread response in the body and it is proposed that Endometriosis is a systemic disease (3). The pain system response includes changes in the central and peripheral nervous system, pelvic organ cross-talk, changes in the pelvic floor and abdominal muscles, alterations in mood, stress and sleep and the presence of comorbid pain syndromes (3,7,8).
Central and Peripheral Sensitisation
Research has shown increases in pelvic nerve size, density, and activity levels in people with EAP (9, 10). This means nerves in the pelvis become excitable and send more ‘danger’ messages to the brain. This neural excitability is not only due to Endometriosis lesions, but also due to a widespread sensitised state – like when an alarm goes off with a minor trigger (like a leaf falling onto a car, setting off the car alarm). Over time, this causes the brain to be bombarded with ‘danger’ signals from the pelvic region, and it loses its ability to dampen down the ‘noise’ from below (descending inhibition). When patients are in this sensitised state, their pain threshold reduces throughout the whole body, meaning they are more sensitive to light, sound, touch, temperature, and smell (11). It can also lead to interpreting normal bodily sensations as a danger or ‘threat’ and may cause discomfort with digestion or bladder filling. When amplification of normal internal sensations causes internal pain, this is referred to as visceral hypersensitivity. (8) The ‘danger’ alarm and a sensitised pain system can be explained to patients using the following image.

Image: Therapeutic Neuroscience Education
Pelvic Organ Cross-Talk
The pelvis is a busy area, housing the bladder, bowel, sex organs, pelvic joints and muscles. Visceral structures (uterus, bowel, and bladder) and somatic structures (skin, muscles, fascia, and bones) in the pelvis share neural pathways before travelling up to the brain (convergence), resulting in similar symptoms. When one area becomes sensitive, resulting in an increase in nerve action, it easily spreads to another neighbouring area, causing it to become excited or sensitive (cross-sensitisation). This pelvic organ cross sensitisation or ‘cross-talk’ is one of the reasons bladder, bowel symptoms and pelvic muscle dysfunction co-exists with EAP (8,9,10). Pelvic organ ‘cross-talk’ via visceral and somatic convergence pathways are illustrated in the image below (12).

Image: Frawley & Peterson (2022)
Pelvic Floor and Abdominal Muscle Function
Research has shown that women with EAP are more likely to have increased tone and tenderness of their pelvic floor and abdominal muscles (13). In fact, in an observational study 45% of Endometriosis patients were not able to completely relax their pelvic floor muscles when assessed (13). This is called pelvic floor tension myalgia – where the pelvic floor muscles are tight and painful to touch and are unable to relax or incompletely relax (14). Symptoms associated with pelvic floor tension myalgia are pain with penetrative sex (dyspareunia), genital aches or sharp pains, voiding dysfunction or defecation difficulty (dyschezia).
Alterations in Mood, Stress and Sleep
Research has shown a depressed mood, anxiety, poor sleep quality, pain anticipation and catastrophising, stress and increased attention to pain are all associated with higher pain intensity (15). This relationship with these factors and endometriosis is thought to be bi-directional, meaning endometriosis and inflammation can alter mood, while stress/anxiety and maladaptive pain beliefs can amplify EAP (15). This is often referred to as the vicious cycle of pain and explains why it is important to address the psychological and emotional distress often experienced in EAP.
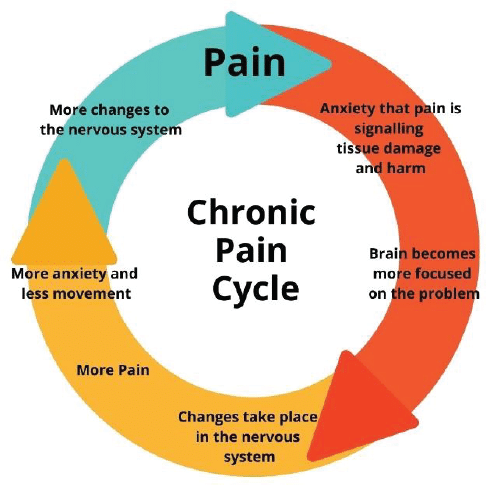
Image: Capital Area Physical Therapy and Wellness
Co-existing Pain Conditions
Women with endometriosis are likely to experience additional chronic overlapping pain conditions, such as bladder pain syndrome (BPS) and irritable bowel syndrome (IBS) (8, 16). In fact, 43 – 60% endometriosis patients were observed to have co-existing BPS which is characterised by pain in the bladder or pelvis, urinary urgency, frequency (17,18). The rate of irritable bowel syndrome (IBS) for women with EAP is 60% (19), and 11% have co-existing vulvodynia (20). All these pain conditions share the common features of pain mediated by inflammation, central and peripheral sensitization, visceral hypersensitivity, and a consequent reduction in quality of life (QOL).
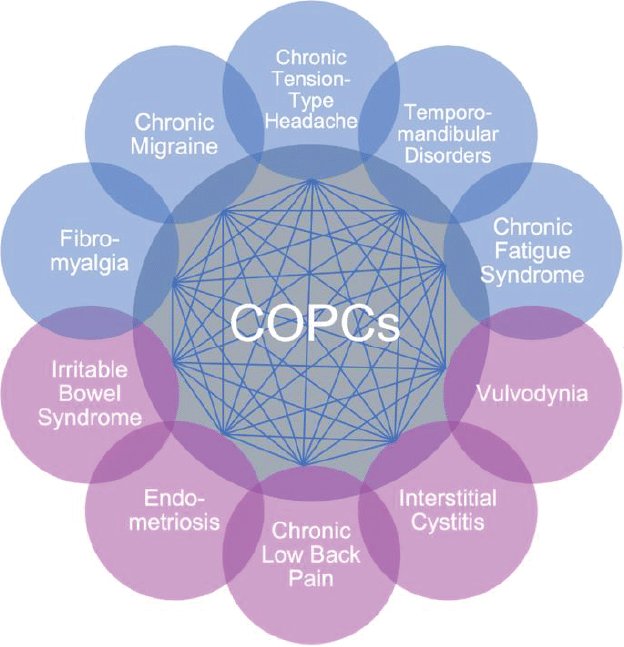
Image: Chronic overlapping pain conditions (COPCs)
Although this presents a complex picture for EAP syndrome, with many different factors beyond lesions influencing one’s pain experience, it is important to remember that all the systems in the body are capable of change (bioplasticity) at any point in the journey. Pelvic Health Physiotherapists with training in gynaecological, urological, and gastroenterological conditions, abdomino-pelvic disorders, general musculoskeletal disorders and persistent pain management, are ideally placed to contribute to the multidisciplinary team approach. Pelvic Health Physiotherapists utilise many different management strategies to support people with EAP to move towards their meaningful goals, they are summarized in the image below (12).
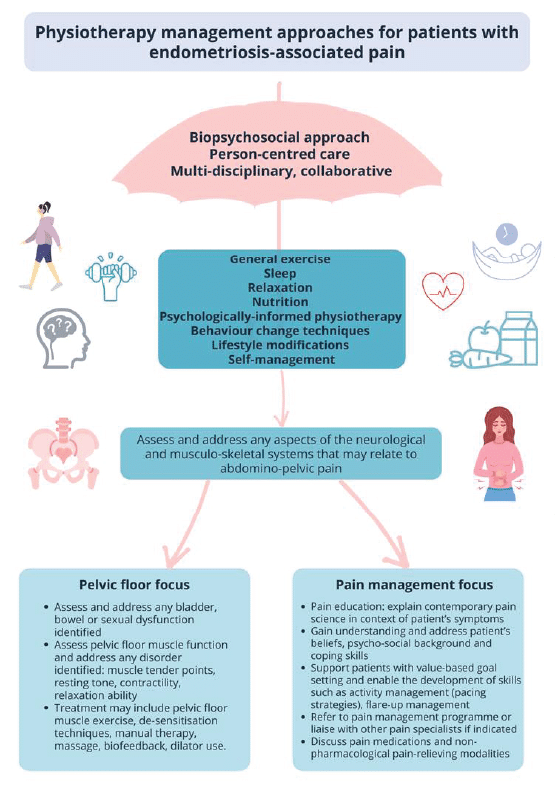
Image: Frawley & Peterson (2022)
The key is to identify what factors are influencing your patient and work with a team of skilled and supportive healthcare professionals to help you manage them. An EAP management toolkit often includes contemporary pain neuroscience education, movement and exercise therapy, mindfulness and stress reduction, pelvic floor muscle treatments, sleep, self-care, dietary changes and psychology. Overtime, this broader, more holistic approach, can reduce pain, improve quality of life and help patients live well with a complex persistent pain condition.
Author
Dr Angela James FACP, Specialist Women’s, Men’s & Pelvic Health Physiotherapist (as awarded by the Australian College of Physiotherapists 2022).
Angela is an active member of the Clinical Advisory Council for Endometriosis Australia.
Acknowledgement
Special mention to Elise Fraser MACP, Lecturer and co-ordinator of WMPH Programs at University of Melbourne, for her contributions to this article.
References
1. Zondervan KT, Becker CM and Missmer SA (2020) Endometriosis, The New England Journal of Medicine, 382:1244–56
2. Rowlands IJ, Abbott JA, Montgomery et al. (2021) Prevalence and incidence of endometriosis in Australian women: a data linkage cohort study. BJOG. 128:657–65.
3. Taylor HS, Kotlyar AM and Flores VA (2021) Endometriosis is a chronic systemic disease: clinical challenges and novel innovations, The Lancet, 397:839–52, doi.org/10.1016/s0140-6736(21)00389-5
4. Armour M, Sinclair J, Ng CHM, et al (2020) Endometriosis and chronic pelvic pain have similar impact on women, but time to diagnosis is decreasing: an Australian survey. Scientific Reports 10:16253
5. Hsu AL, Sinaii N, Segars J, Nieman LK et al. (2011) Relating Pelvic Pain Location to Surgical Findings of Endometriosis. Obstet Gynecol. 201, 118(2 Pt 1), 223–230.
6. Engler et al. (2023) EAU Guidelines on Chronic Pelvic Pain. Accessed online https://uroweb.org/guideline/chronic-pelvic-pain/
7. Yong PJ, Williams C, Behaiwy MA and Allaire C. (2020) A Proposed Platform for Phenotyping Endometriosis-AssociatedPain:UnifyingPeripheralandCentralPainMechanisms. CurrentObstetricsand Gynecology Reports. 9:89-97
8. McNamara HC, Frawley HC, Donoghue JF et al. (2021) Peripheral, Central, and Cross Sensitization in Endometriosis-Associated Pain and Comorbid Pain Syndromes: Frontiers in Reproductive Health.
9. Maddern J, Grundy L, Castro J and Brierley SM (2020) Pain in Endometriosis. Front Cell Neurosci
10. ZhengP,ZhangW,LengJandLangJ.(2019)Researchoncentralsensitizationofendometriosis-associated
pain: a systematic review of the literature. Journal of Pain Research. 12: 1447-1456
11. NijsJ,GeorgeSZ,ClauwDJ,Fernández-de-las-PeñasC,KosekE,IckmansKetal.(2021)Central
sensitisation in chronic pain conditions: latest discoveries and their potential for precision
medicine. Lancet Rheumatol 3:e383-92
12. FrawleyH&PetersonK(2022)PhysiotherapyforEndometriosis.Globallibraryofwomen’smedicineISSN:
1756-2228
13. FragaMV,etal.(2021)Pelvicfloormuscledysfunctionsinwomenwithdeepinfiltrativeendometriosis:An
underestimated association. Int J Clin Prac;75(8):e14350.
14. FrawleyHetal(2021)AnInternationalContinenceSociety(ICS)ReportontheTerminologyforPelvic
Floor Muscle Assessment. Neurourol Urodyn.
15. McPeakAE,etal.(2018)PainCatastrophizingandPainHealth-RelatedQuality-of-Lifein
Endometriosis. Clin J Pain;34(4):349–56
16. LamvuG,etal.ChronicPelvicPaininWomen:AReview.JAMA2021;325(23):2381–91.
17. TirlapurSA,KuhrtK,ChalihaC,BallE,MeadsC,KhanKS.(2013)The’eviltwinsyndrome’inchronicpelvic
pain: a systematic review of prevalence studies of bladder pain syndrome and endometriosis. Int J Surg.
18. ChengC,RosamiliaA,HealeyM.(2012)Diagnosisofinterstitialcystitis/bladderpainsyndromeinwomen
with chronic pelvic pain: a prospective observational study. Int Urogynecol J.
19. SchomackerML,HansenKE,Ramlau-HansenCH,FormanA.(2018)Isendometriosisassociatedwith
irritable bowel syndrome? A cross-sectional study. Eur J Obstetr Gynecol Reprod Biol.
20. GraziottinA,MurinaF,GambiniD,TaraborrelliS,GardellaB,CampoM.(2020)Vulvarpain:therevealing
scenario of leading comorbidities in 1183 cases. Eur J Obstetr Gynecol Reprod Biol.